Pathophysiology
Under the broader category of Dystrophy. This is an X linked recessive disease. Caused by the deletion of the short arm of the chromosome 21. Due to the mutation, a protein called dystrophin becomes deficient.
Dystrophin is a protein that helps connect the extracellular matrix of the muscle cells to the cytoskeleton through the cell membrane.
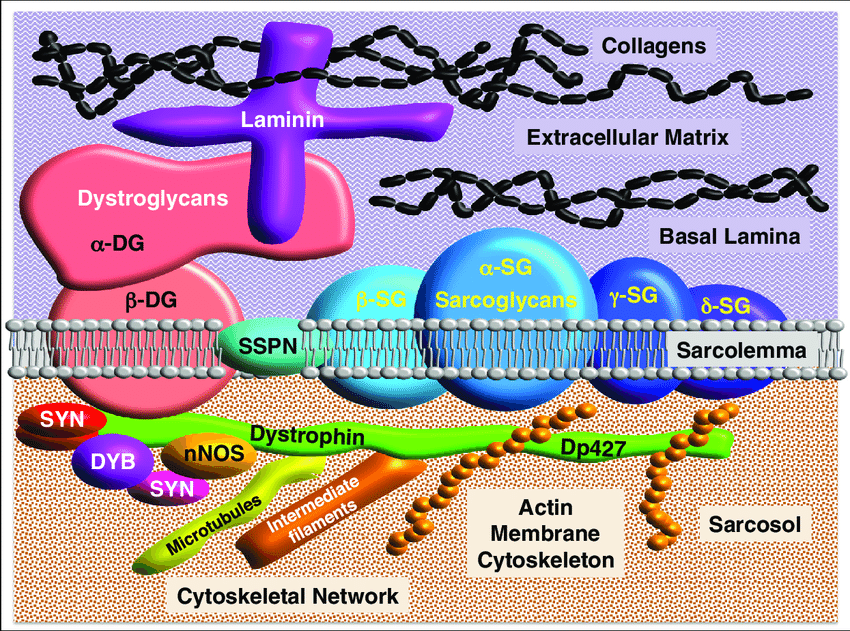
Dystrophin is essential for cell membrane stability. Deficiency leads to reduction in three glycoproteins (α-, β- and γ- sarcoglycans) in the dystrophin- associated protein complex (DAP complex) that links dystrophin to laminin within cell membranes.
As a result, the sarcolemma becomes fragile, more susceptible to micro-tears or disruptions during the normal mechanical stress of muscle contraction/relaxation.
Once the sarcolemma is destabilized, there is an influx of ions into the cell, this causes activation of proteolytic enzymes and also causes the damage of organelles. This causes necrosis of the myofibrils. Due to the myofibril necrosis, Creatine Phosphokinase (CPK) level is increased.
Clinical Features
Children present with waddling gait and/or language difficulty. On average, this is seen when they reach about 5.5 years. Life expectancy is about 20 years with the disease but with modern therepy now it has gone up to 40 years. There is no cure, diseases progression can be delayed.
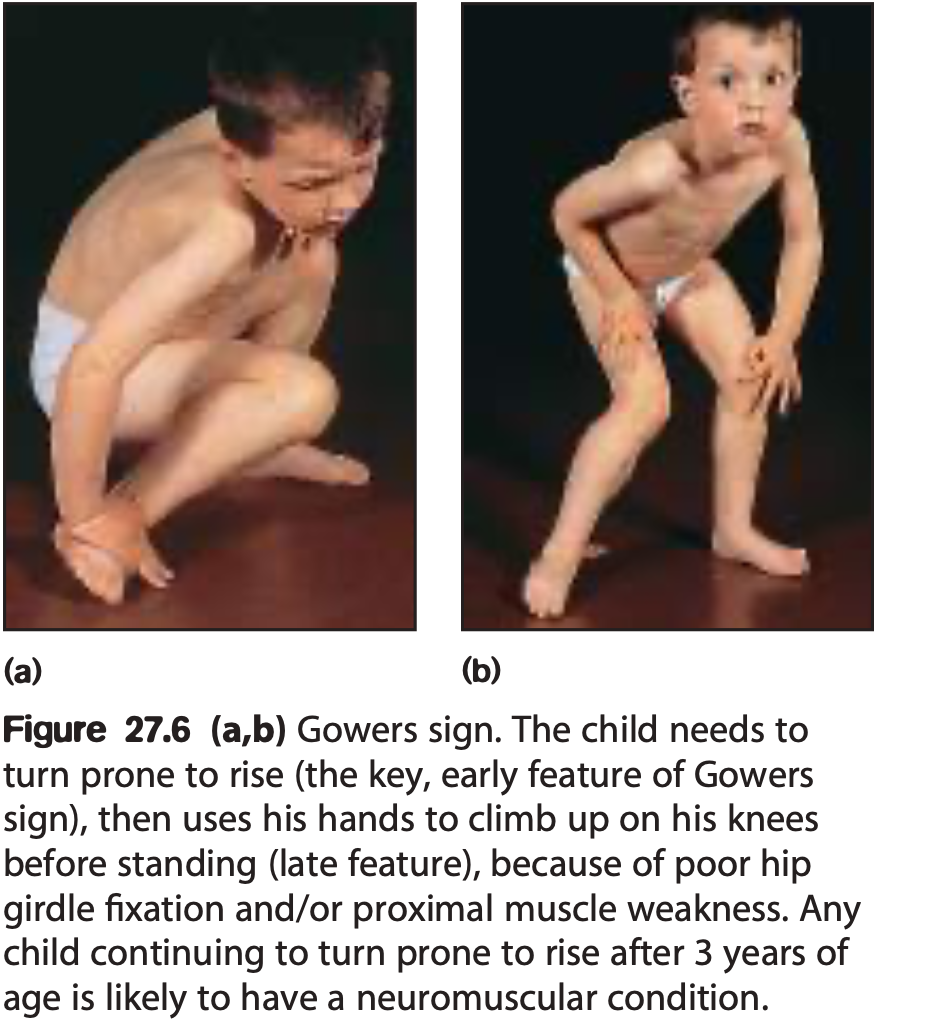
From early childhood, Gower’s sign is seen. Pseudo hypertrophy of the calves occur due to replacement of muscle fibers with fat and fibrosis in the muscles.
DMD is associated with cardiomyopathy and later in life death occurs mainly due to it or respiratory failure.
There is no curative treatment but new gene- editing therapies are in development. Steroids may delay progression. Physiotherapy helps prevent contractures in the later stages. Non- invasive respiratory support and multidisciplinary care improve life expectancy. Carrier detection. Females with an affected brother have a 50% chance of carrying the DMD gene. In carriers, 70% have a raised CK, and usually EMG abnormalities and/or changes on biopsy. Carrier and prenatal diagnosis is available with genetic counseling.